


Introduction
Methods
Patient positioning and preparation
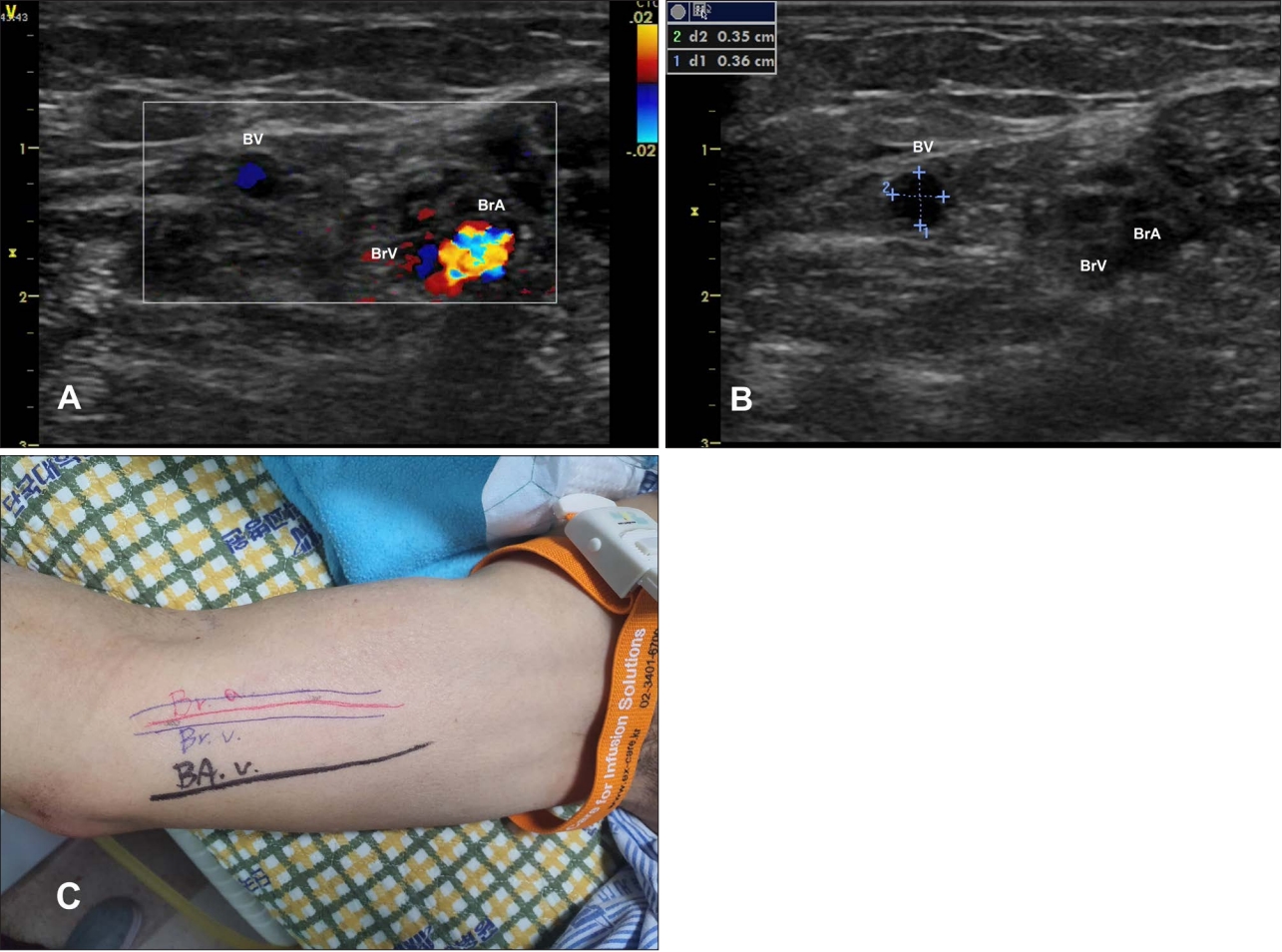
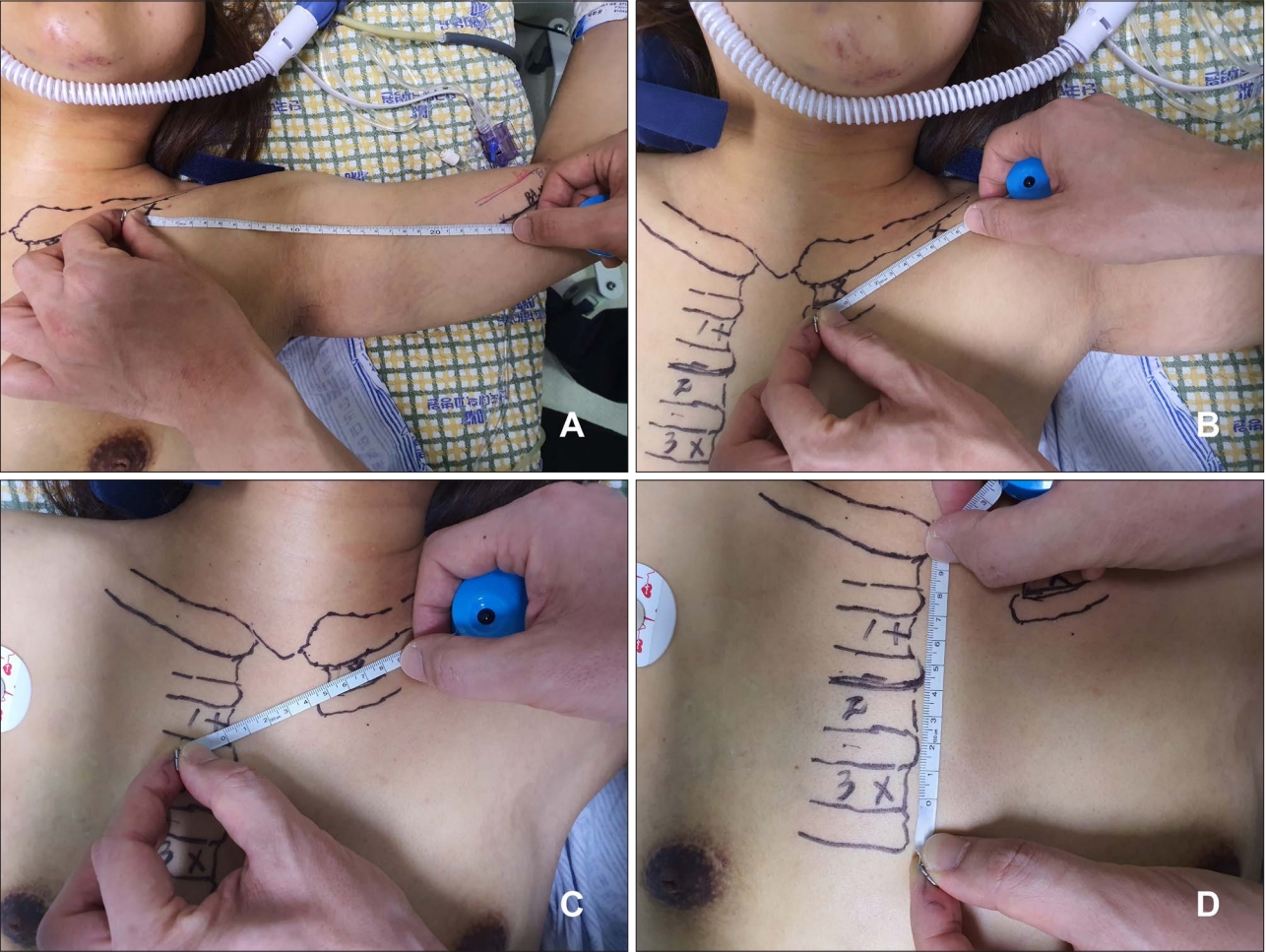
Venous assessment and measurement
Preparation of the PICC
Procedure
1. The basilic vein puncture is performed using a 21-gauge micropuncture needle (7 cm in length) under ultrasound guidance.
2. A 0.018-inch guidewire (50 cm in length) is introduced into the vein through the needle.
3. The location of the guidewire in the vein is confirmed by ultrasonography, and the tourniquet is released.
4. The needle is then withdrawn, and 2% lidocaine is injected into the skin around the puncture point.
5. An incision to accommodate the sheath microintroducer is made at the puncture point using a scalpel.
6. With its inner dilator, the short peel-away sheath microintroducer is advanced along the guidewire into the vein, with the wire and dilator removed.
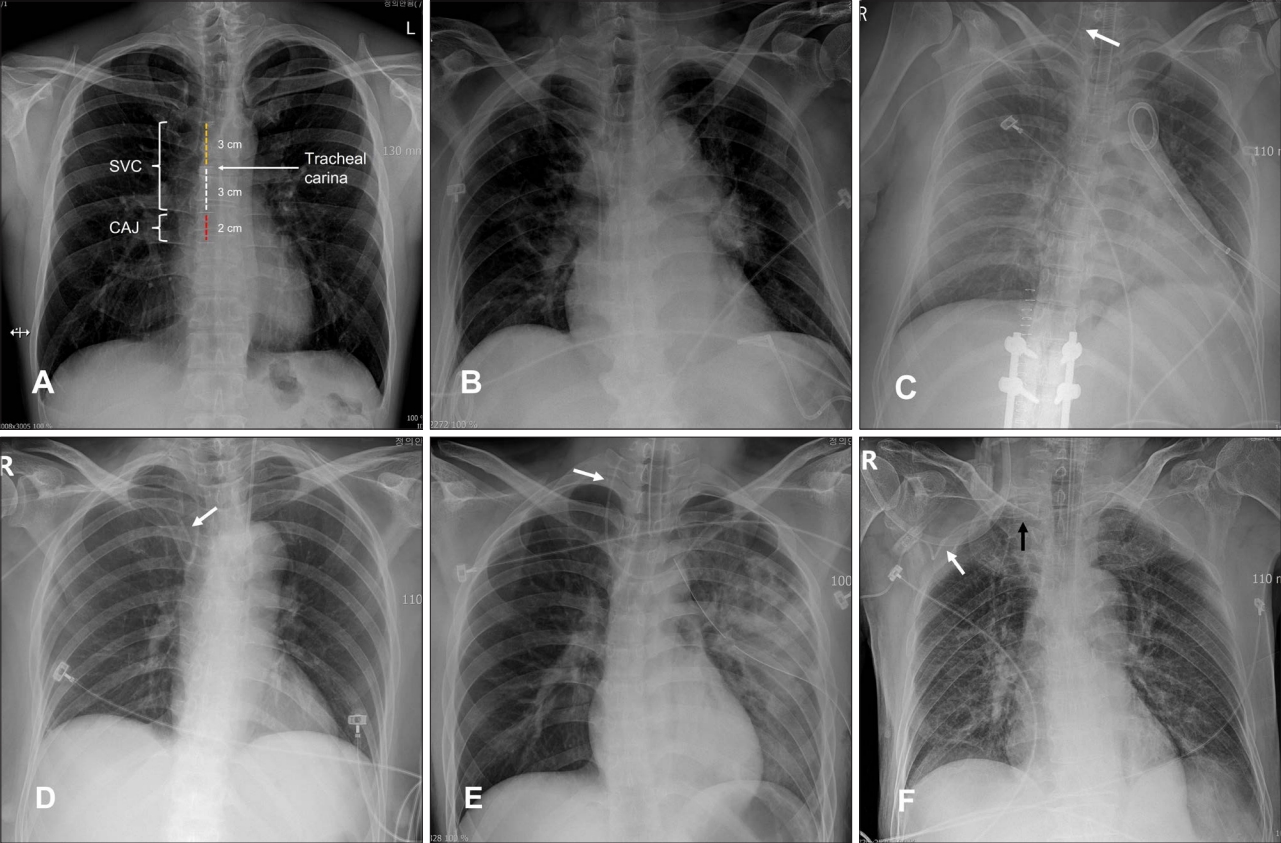
7. The 5 Fr catheter (55 cm in original length) is introduced into the vein through the sheath. If the patientŌĆÖs head cannot be turned ipsilaterally, the catheter can be advanced further while pressure is applied by the operatorŌĆÖs left hand near the confluence of the ipsilateral internal jugular vein (IJV) and the subclavian vein.
8. The sheath is peeled away and removed after absence of the catheter in the ipsilateral IJV is confirmed by ultrasonography. If the catheter is in the IJV, it is pulled back and advanced again.
9. Of two lumens, blood reflux through the red lumen in which the stylet (80 cm in length) is not mounted is checked using a syringe at first. The lumen is then flushed with saline.
10. After the three-way connector holding the stylet in the blue lumen has been removed, blood reflux is again checked, and the lumen is flushed.
11. Both lumens are locked with the disinfection caps.
12. The hub of the PICC is secured using a sutureless stabilization device (in this case, a StatLock® PICC Plus: Bard Venetec International, San Diego, CA, USA). A transparent gel pad integrating chlorhexidine gluconate is used as a dressing.