


Introduction
Visceral artery aneurysms (VAAs) and visceral artery pseudoaneurysms (VAPAs) are relatively rare. Traumatic pseudoaneurysms arising from the branches of the superior mesenteric artery (SMA) are rarely reported; however, they are clinically important lesions because of the risk of hemorrhage and bowel ischemia [1].
Herein, we present the case of a patient with an SMA branch pseudoaneurysm associated with blunt trauma.
Case presentation
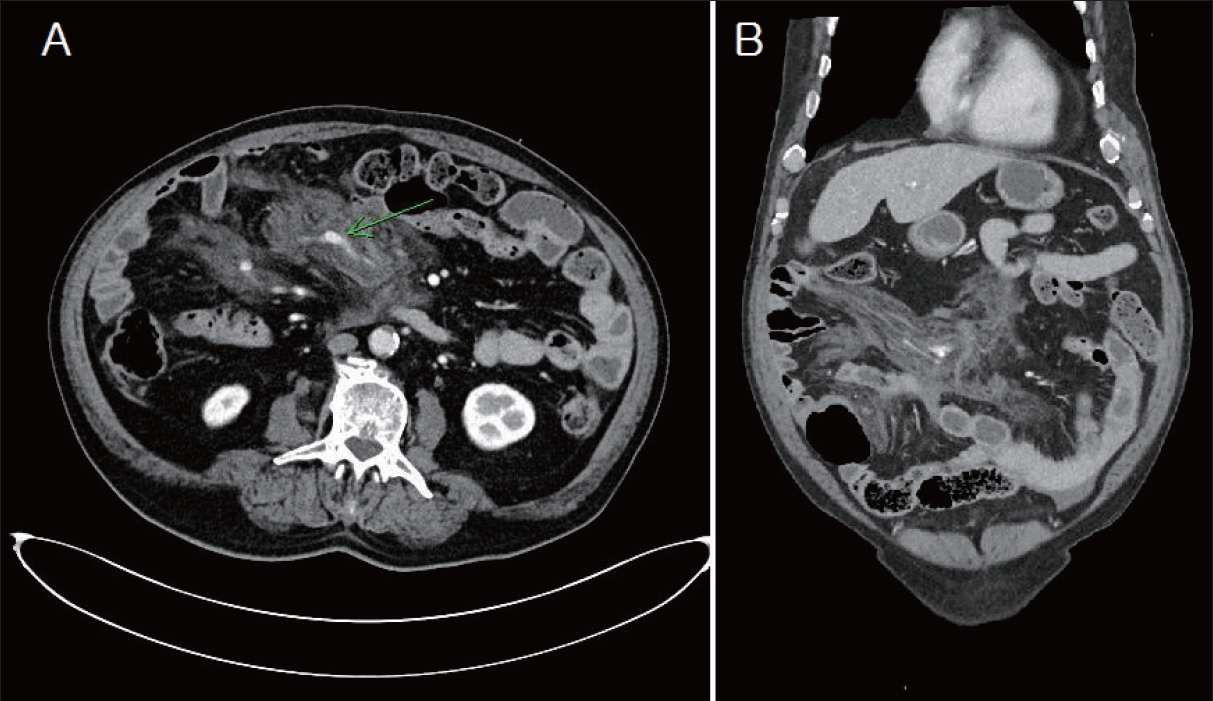
A 77-year-old man with hypertension, diabetes, and dyslipidemia came to our trauma center after a car accident. He complained of abdominal pain and left chest wall pain, and computed tomography (CT) revealed ileal mesenteric injury with active arterial extravasation and hematoma (Fig. 1). An emergency laparotomy was performed, and serosal tear, perforation of the jejunum, and rupture of the mesentry were repaired. In addition, the patient had Jefferson fracture type III, multiple rib fractures, hemothorax, and hemopericardium. After surgery, acute kidney injury and rhabdomyolysis occurred during conservative treatment and were treated with continuous renal replacement therapy. On the 38th hospital day, the patient’s condition improved and he was transferred to a lower-level hospital.
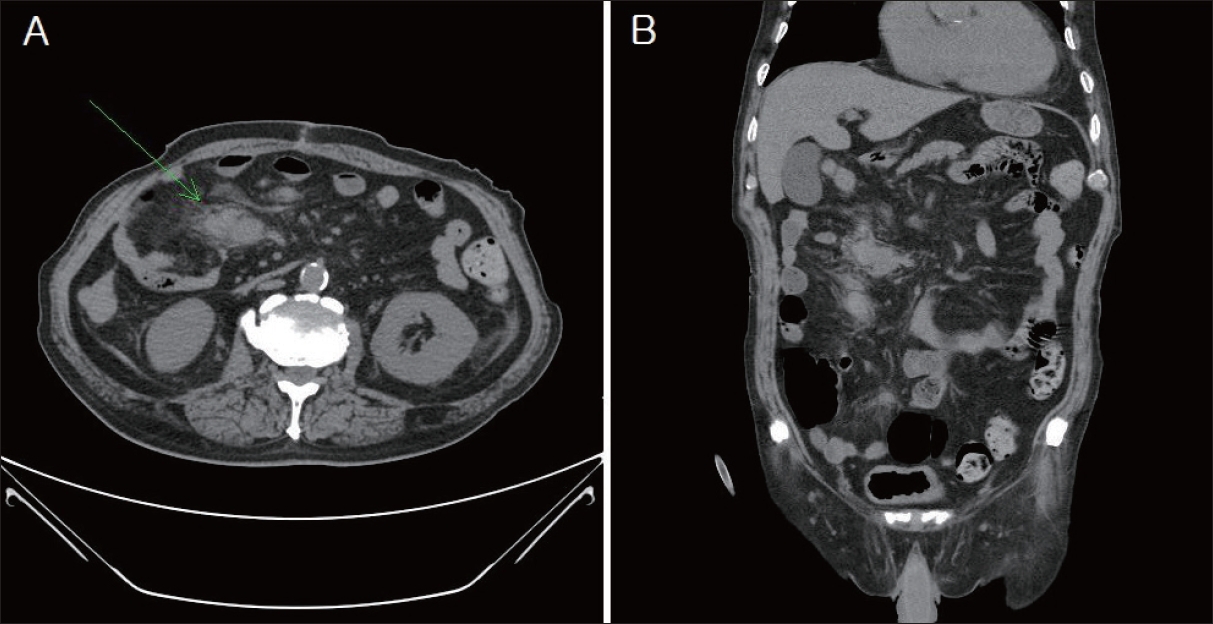
Approximately 1 month after transfer, the patient complained of abdominal pain and distension. CT performed at the hospital where he was transferred detected a pseudoaneurysm in an SMA branch. The pseudoaneurysm was located in the area where the hematoma was observed in the previous trauma, and he was transferred to our hospital again (Fig. 2). He had no symptoms other than mild fever and abdominal pain, and his vital signs were stable. On the day of admission, laparotomy was performed because of a pseudoaneurysm accompanied by inflammation. When vascular embolization was performed, the risk of additional complications, such as intestinal necrosis, was considered. After the excision of the pulsatile mass, the bleeding site was ligated and the small bowel with ischemic changes was segmentally resected (Fig. 3).
Discussion
VAPAs can be a result of trauma, surgery, or infection; their rupture constitutes an abdominal emergency. Because these are rare aneurysms, the rate of rupture of SMA branch aneurysms is unknown. Although the rupture risk is thought to be low, the mortality rate associated with the rupture ranges from 20% to 40% [2,3]. VAPAs represent essentially a contained rupture that is only constrained by a fibrous capsule because all three layers of the arterial wall are disrupted. Compared with true aneurysms, pseudoaneurysms have a higher risk of overt rupture; thus, VAPAs are typically treated when identified. Depending on the diameter and location, pseudoaneurysm rupture is associated with a mortality rate ranging from 25% to 70% [4]. As mentioned earlier, VAAs/VAPAs are very rare and not all traumatic artery damage results in pseudoaneurysm formation. In this case, despite the successful repair of the initial damage, a pseudoaneurysm was formed over time because of traumatic visceral arterial injury. A noncontrasted abdominal CT performed on the 16th hospital day during the first admission showed a lesion suggestive of pseudoaneurysm (Fig. 4). However, this is a retrospective analysis, and at that time, it was just considered an improving state of mesenteric damage.
Therefore, in the follow-up of patients with visceral arterial injuries, re-evaluation via CT should be considered if necessary. Open surgical repair and reconstruction may remain the optimal strategy for some VAAs/VAPAs, particularly in patients with unstable hemodynamics and requiring emergency repair [5]. In other cases, endovascular intervention may be considered.