


Introduction
Gastric injury after blunt trauma is well known for its rarity. The incidence is reported to be <2% of all blunt abdominal trauma [1]. Laparoscopic exploration for blunt trauma is known to be safe in patients with stable hemodynamics [1,2]. However, continuing a laparoscopic procedure can be unsafe in some cases, requiring conversion to laparotomy. Herein, we present a case of a laparoscopic exploration converted to laparotomy because of the massive spillage of gastric contents.
Case presentation
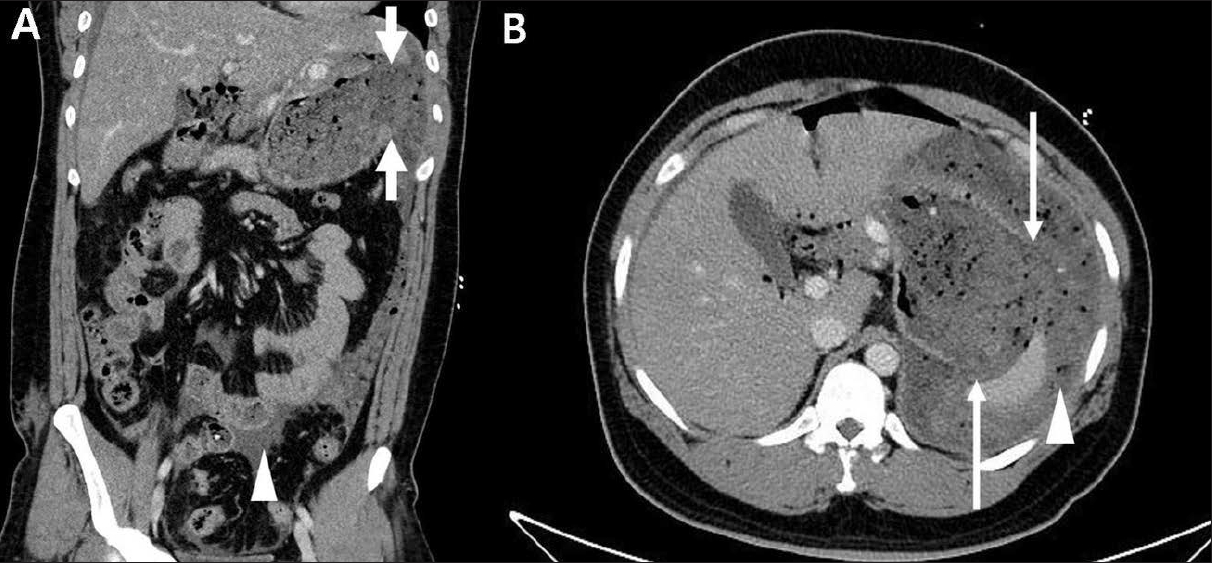
A 29-year-old man was transferred to the emergency department after being crashed by a cow’s head. His initial vital signs were stable, except for tachycardia (a heart rate of 125 beats per minute), with alert mentality. On physical examination, tenderness and rebound tenderness on the whole abdomen with rigidity were observed. In the focused assessment with sonography for trauma, intraperitoneal injuries were highly suspected because large amounts of free fluid were found in Morison’s pouch and the splenorenal recess. Preoperative computed tomography (CT) revealed a wide gastric wall defect from the gastric fundus to the upper body, a focal subcapsular laceration in the spleen, and multiple left-sided rib fractures (Fig. 1). The patient had stable hemodynamics; therefore, laparoscopic surgery was performed to investigate and control the injuries. During laparoscopic inspection, huge amounts of food materials disseminated throughout the abdomen were found (Fig. 2). A rupture measuring 15 cm was found on the greater curvature of the gastric upper body. Although the lesion was treatable with an endostapler and the patient had stable hemodynamics, the operation was converted to laparotomy without hesitation because food residues were found throughout the abdominal cavity, and it was nearly impossible to access the lesion and handle the devices. Wedge resection, bleeding control of the spleen, and evacuation of food materials via copious irrigation of 15,000 mL of saline were performed successfully via laparotomy. The patient was discharged on postoperative day 14 without any complications.
Discussion
The small bowel is the most commonly injured intraperitoneal hollow viscus after blunt traumas [2]. Isolated gastric rupture caused by blunt traumas occurs rarely, with incidences ranging from 0.02% to 1.7% of all abdominal blunt trauma cases. Similar to other abdominal blunt traumas, gastric ruptures are mainly caused by traffic accidents [1]. A thick wall, muscularity, mobility, and protective position of the stomach contribute to resistance to blunt traumas when the organ is empty. However, if the stomach is expanded by a recently trapped meal, it can be easily injured by an external force. The mechanism of blunt gastric injuries involves an abrupt surge in intragastric pressure due to the external force, which can result in gastric rupture [1].
Thus far, indications are unclear for the laparoscopic exploration of blunt abdominal traumas, except for hemodynamic stability [3-5]. However, studies are even rarer for blunt gastric injuries than for other blunt abdominal injuries; only several case reports have been published [6]. In fact, massive food material spillage can also be indicated for the following reasons: First, the injured site can be covered up, making it invisible and inaccessible. Second, the surgeons cannot perfectly remove food soiling. The larger and thicker the particles, the more difficult the procedure becomes. Third, irrigation with laparoscopic devices is even more difficult, increasing the possibility of postoperative infection. A recent retrospective cohort study proved that the laparoscopic procedure in patients with severe peritoneal soiling, such as bowel contents, was more likely to be converted to open surgery [7].
We experienced a case of laparoscopy converted to laparotomy in a patient with gastric rupture after a blunt trauma. If surgeons suspect massive food material spillage from the injured stomach in the preoperative examination, such as CT, laparotomy should be considered instead of laparoscopy even if the patient is hemodynamically stable. If an unexpectedly large amount of food spillage is encountered during laparoscopy, conversion to laparotomy is necessary.