


Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease. The systemic inflammation of multiple organs caused by autoantibodies varies in severity from mild inflammation to potentially life-threatening diseases [1,2].
Delayed perforation of the small bowel after blunt trauma is extremely rare [3]. However, clinicians should stay alert about the possibility of delayed (or not detected) bowel injuries in a patient who complains of abdominal pain with nonspecific findings in the radiological tests. Specifically, patients with systemic inflammation require more attention because it can result in systemic vasculature insufficiency.
Herein, we report the case of a patient with SLE who was transferred after sustaining a blunt trauma. Small bowel injuries were suspected; however, the findings to determine the need for an emergency operation were unclear. Forty-eight hours after admission, the patient complained of high fever with mild abdominal pain, and abdominal computed tomography (CT) revealed pneumoperitoneum with bowel injuries.
Case presentation
A 38-year-old man was transferred to our institution after sustaining burn injuries and falling from a height of 5 m. He had set his apartment on fire and fallen through the window. The patient had suffered from psychosis because of a high-grade SLE with brain involvement and was taking high-dose steroids. He also had chronic cholecystitis but had refused cholecystectomy. After arrival, the patient complained of back pain, right ankle pain, and mild abdominal pain. However, the findings of the physical examination of the abdomen were not specific.
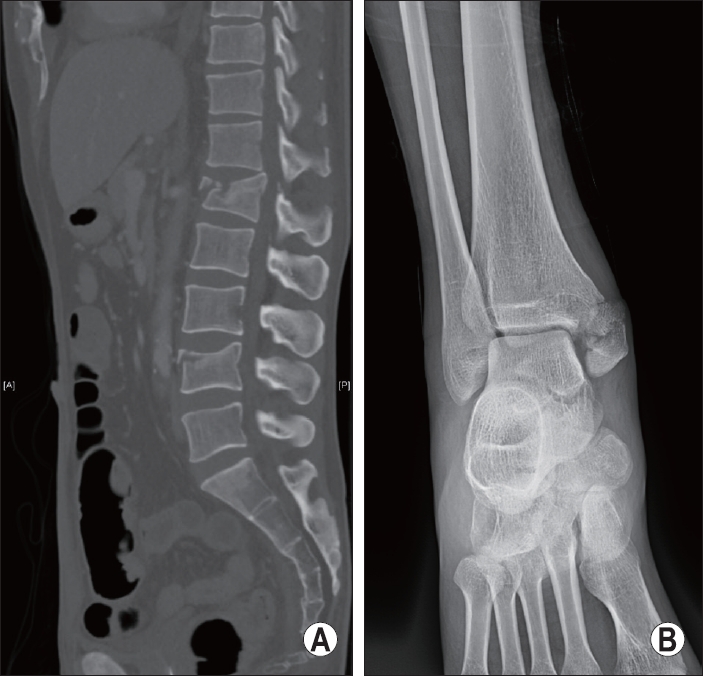
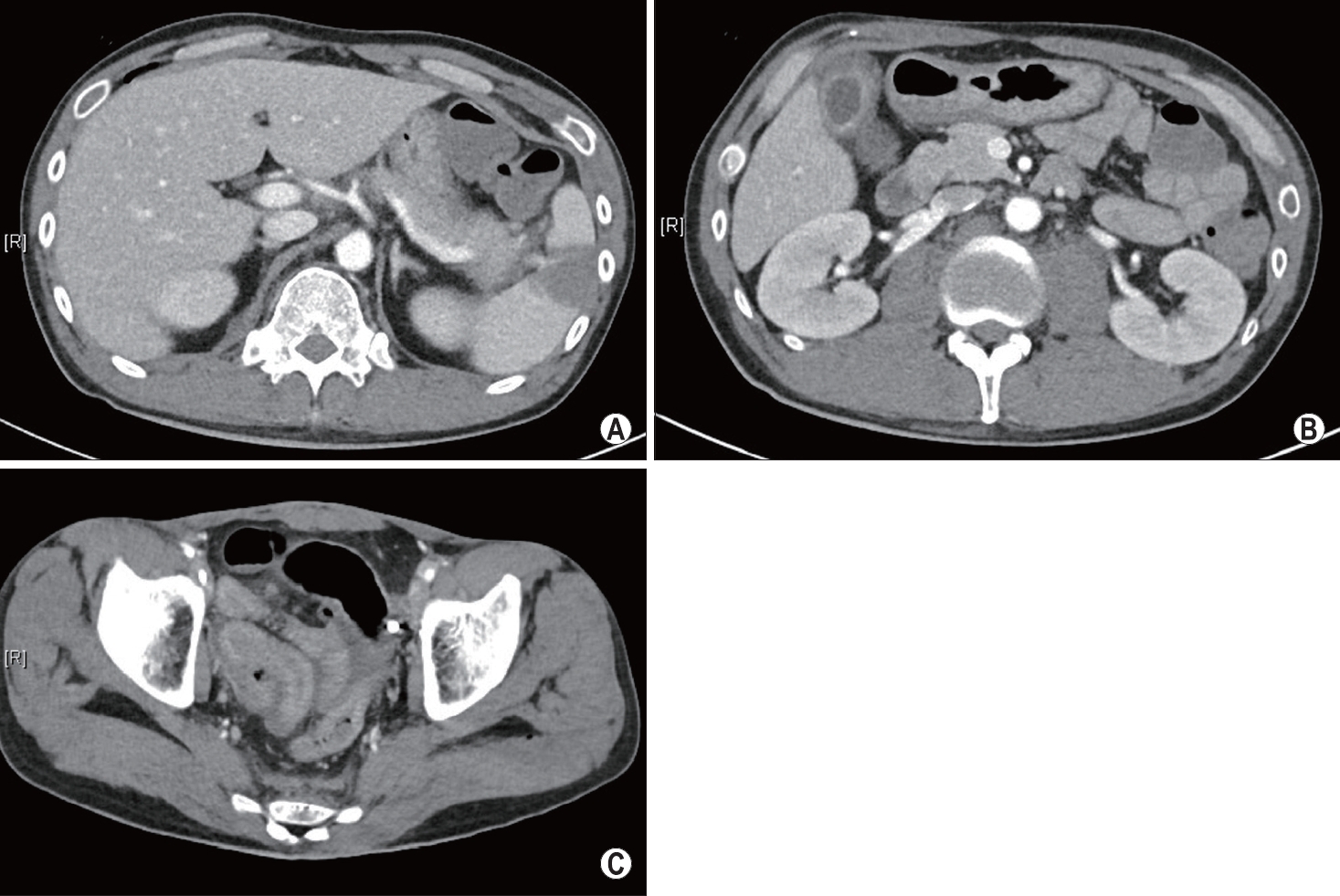
At the initial abdominal sonography, no fluid collections were noted in the intra-abdominal spaces. Radiological tests revealed multiple fractures of the lumbar spine and comminuted fracture at the right medial malleolus (Fig. 1). Abdominal CT revealed grade 2 splenic injury [4], chronic cholecystitis, and a small amount of fluid collection in the pelvic cavity without pneumoperitoneum (Fig. 2). Fluid collection in the pelvic cavity may indicate small bowel injuries. However, it was not easy to determine whether emergency laparotomy was necessary because of the known cholecystitis and nonspecific findings of the physical examinations. After consultation with radiologists, we thought that the fluid collection detected via abdominal CT might be due to spleen injury. In addition, as lumbar spine fractures require urgent surgery, a close observation was initiated for the possibility of small bowel injury.
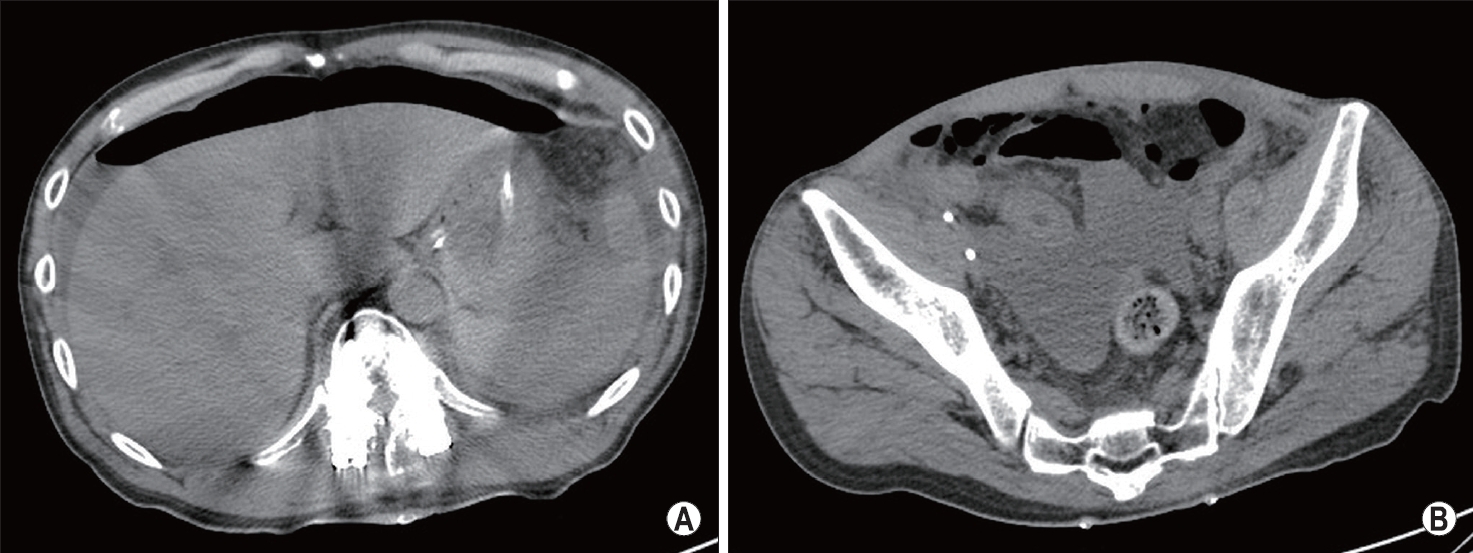
The patient was admitted to the intensive care unit after the emergency posterior lumbar interbody fusion surgery of the lumbar spine. After 48 h from admission, the patient complained of abdominal pain with direct and rebound tenderness. Follow-up abdominal CT was performed immediately, which detected pneumoperitoneum at subphrenic spaces and fluid collection in the pelvic cavity (Fig. 3).
Consequently, emergency laparotomy was performed. Small bowel perforation with focal necrosis and 20 cm of mesenteric tear at a site 170 cm from the ileocecal valve was found (Fig. 4). Segmental resection with end-to-end anastomosis of the perforated small bowel was performed. Additional splenectomy and cholecystectomy for the spleen injury and chronic cholecystitis were performed. After the emergency operation, the patient was transferred to the department of rheumatology for the treatment of SLE without other complications at 18 hospital days and 16 postoperative days.
Discussion
CT is a potent tool for detecting pneumoperitoneum [5]. However, small bowel injuries are often difficult to detect on CT. Only approximately 50% of the pneumoperitoneum caused by small bowel injury are detected with CT [5,6].
SLE is an autoimmune disease with systemic inflammation in multiple organs. In many systemic autoimmune diseases, systemic blood flow is impaired because of atherosclerotic changes in the vessels [7]. Moreover, vascular problem caused by systemic inflammation and the use of steroids could accelerate the necrosis [8,9]. The necrosis of the small bowel was severe although only 2 days had elapsed after the injury.
In this patient, delayed perforation of the small bowel was caused by mesenteric injury; however, diagnosis was difficult because of the confused mental status of the patient and unclear results of abdominal CT and physical examinations. Furthermore, the patient’s medical history (i.e., SLE and chronic cholecystitis) made the decision difficult. Nonetheless, via history taking, his vasculature was predicted to be poor and that the necrosis would rapidly worsen. With serial checking, signs of generalized peritonitis were detected; finally, the small bowel injury was diagnosed.
Diagnosis of damage to the small bowel without free air on the abdominal CT is difficult; nevertheless, delayed diagnosis worsens the prognosis. Therefore, continuous physical examination and immediate and follow-up im-aging tests are essential in cases suspected of small bowel injury even if initial imaging tests reveal negative findings. Any medical history that may aggravate the patient’s condition must be recognized.