A Cecal Perforation in a Blunt Trauma
Article information
Abstract
Immediate cecal perforation in blunt trauma is rare. We experienced a case of perforation of the cecum after a passenger traffic accident, which is reported herein.
CASE
A 65-year-old female underwent passenger traffic accident. She was putting a seat belt. She arrived at authors` emergency department via ground ambulance from other hospital. The patient complained of generalized abdominal pain, and her initial vital signs were blood pressure 101/51 mmHg, heart rate 85, respiratory rate 20, body temperature 36.8℃ and sPO2 97%. A seat-belt sign was seen from her anterior chest wall to lower right abdominal wall. We detected free air and fluid collection in her abdominal cavity of computed tomography scan which was performed at the previous hospital (Fig. 3.). An emergency laparotomy was performed. About 1 L of fresh blood was collected in the abdominal cavity and a moderate amount of bowel spillage was detected. Multiple mesenteric lacerations were identified 190cm distal area from Treitz ligament and 5cm above from IC valve. Omental tearing was also identified. Cecal perforation was noted on the countermesenteric area. We decided one-stage operation. After adequate hemostasis, the omental and mesenteric tearing were repaired primarily. A partial cecaectomy was performed using stapler on the perforation of the cecum (Fig. 2.). The patient was discharged uneventfully.
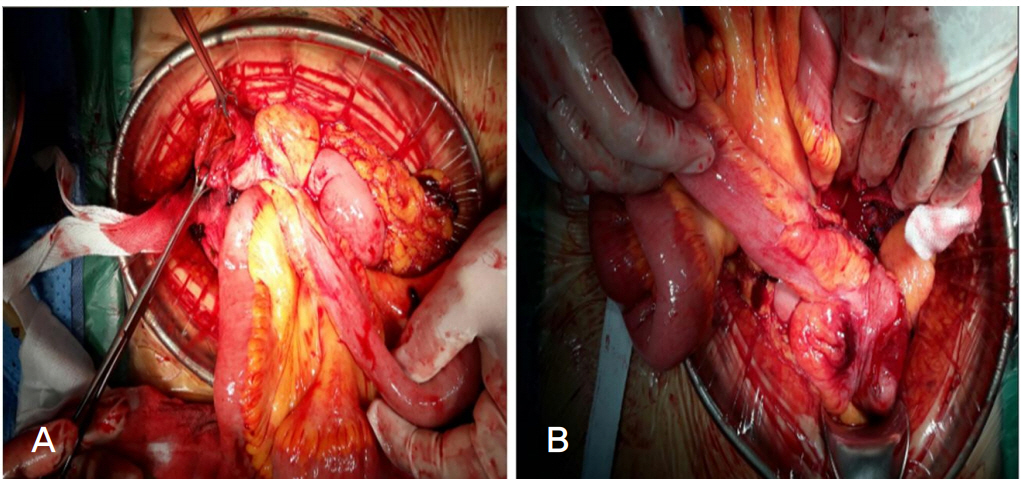
(A) A free perforation was identified. (B) A partial cecectomy was performed using surgical stapler.
DISCUSSION
In a blunt trauma, a cecal perforation is very rare. If the injury is identified without delay, cecal perforation could be managed with one-stage operation [1].
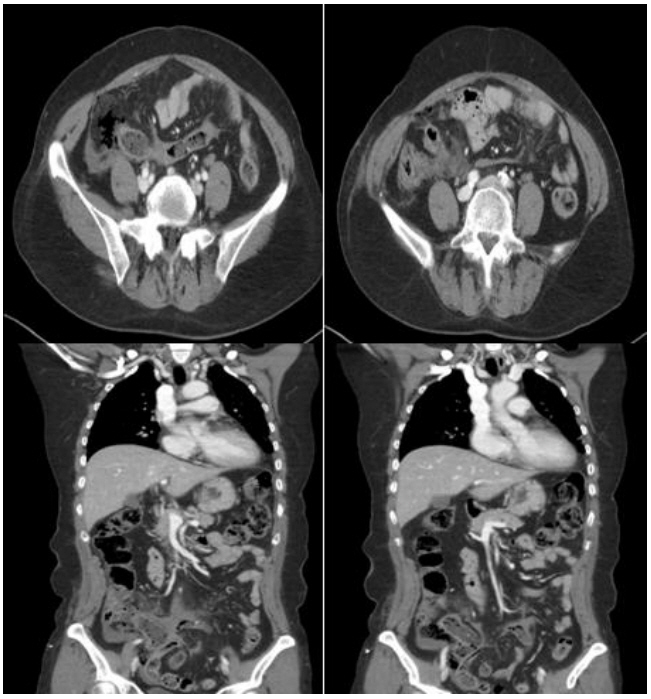
The computed tomography scan shows free air and fluid collection around cecum.
Notes
Conflict of Interest Statement
No potential conflict of interest relevant to this article was reported.