Rib fixation with a plate for radius and overlapping technique in comminuted fractures
Article information
Abstract
A 49-year-old male with sustained multiple comminuted right rib (3rd–9th) fractures, right pneumothorax, and a flail chest was referred with complaints of severe pain. The successful management of the comminuted fractures with a typically used method was deemed not plausible. Therefore, rib fixation was performed using an overlapping technique and plates employed for radius fixation.
CASE
A 49-year-old male with sustained multiple comminuted right rib (3rd–9th) fractures, right pneumothorax, and a flail chest was referred to our hospital with complaints of severe pain. He previously underwent closed thoracostomy in the right thoracic cavity. Rib fixation was performed after 4 days. On evaluation, comminuted fractures of the 4–8th right ribs were detected. We followed a conventional method of using an 8- or 6-hole-plate (MatrixRIB™; DepuySynthes, USA) and an 8- or 4-hole-plate (RibFix Blu™; DepuySynthes) for his rib fixation. The fourth rib was fixed using an 8-hole-plate (MatrixRIB™). However, the distance of the intact portion on the 5–7th ribs was too long to be successfully managed using a conventionally used plate. Therefore, 8-hole-plates (Small Fragment Locking Compression Plate; DepuySynthes), which are usually employed for radius fixation, were used on these ribs. The 8th rib was fixed with an overlapping method with two flexible 4-hole-plates (RibFix Blu™) and a longer screw, considering the anatomy of the comminuted fractures (Fig. 1.). The patient was extubated the day after the operation and was transferred to the general ward on the second day after the operation. The plates were intact even on 40th postoperative day.
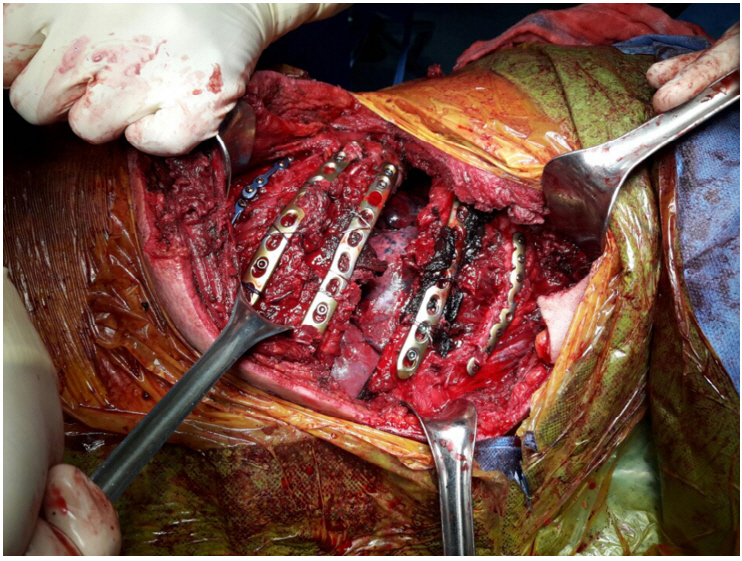
The fourth rib was fixed using an 8-hole-plate (MatrixRIB™). The 5–7th ribs were fixed using 8-hole-plates (Small Fragment Locking Compression Plate, DepuySynthes, USA). The 8th rib was fixed using two flexible 4-hole-plates (RibFix Blu™)
DISCUSSION
Surgical management of patients with rib fractures contributes to significant reductions in pneumonia, the length of hospital stay, and intensive care [1, 2]. Extremely anterior fractures typically cannot be repaired without using costal cartilage as the fixation point. The long-term outcome of costal fixation is unknown. The adequate length for reduction and fixation is typically 3–5 cm on either side of the fracture [2]. Thus, it is a common practice to typically perform fixation using at least ≥2 screws (usually 3) on either side of the fracture for achieving an adequate length for reduction and fixation. Here, the comminuted rib fractures were fixed using the plate for radius and overlapping technique. Thus, a favorable outcome could be anticipated.

Details of the fixation of the 8th rib
Notes
Conflict of Interest Statement
None of authors have a conflict of interest.