


CASE
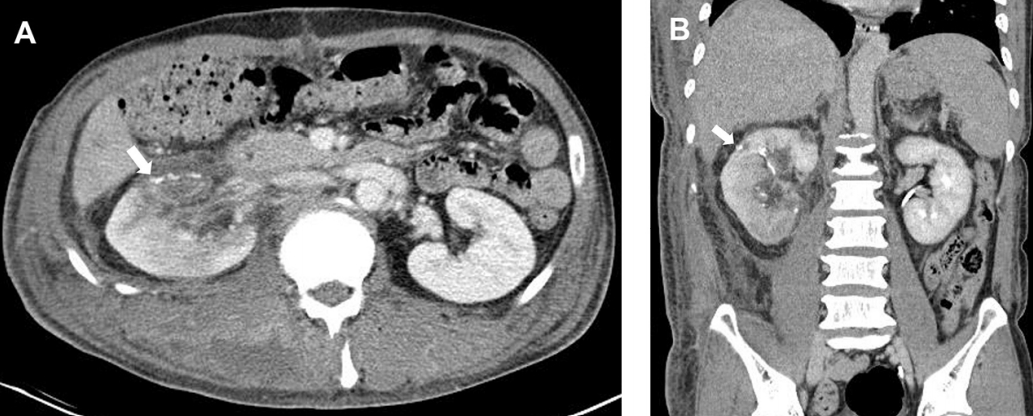
The wire under construction hit the right back of a 56-year-old male (Fig. 1). Upon admission, the patient’s blood pressure was 92/59 mm Hg, pulse rate was 125 beats/min, and he had been transfused with 2 units of packed red blood cell. The focused assessment with sonography for trauma revealed intra-abdominal fluid collection in the Morison pouch. Abdomen computed tomography (CT) performed in response to resuscitation demonstrated multiple laceration at the Couinaud segment V, VI, and VII of the liver, and multiple lacerations deep to the calyx in the right kidney with the contrast extravasation (Fig. 2). The injury severity score was 26. Therefore, he underwent emergency laparotomy due to intermittent hypotension. Right renorrhaphy with temporary renal vascular pedicle clamping after the temporary perihepatic packing was performed with transfusion of 2 units of packed red blood cell during the operation time of 165 min (Video 1), with the clamping time of 20 min at the right vascular pedicle. After the definitive surgery, serum creatinine level decreased from 1.43 mg/dL to 0.88 mg/dL within postoperative day 3. Follow-up abdominal CT on postoperative day 8 demonstrated a well-reconstructed right kidney with normal parenchymal enhancement without significant fluid collection (Fig. 3). He was discharged without any abdomen-related complications on postoperative day 20.
DISCUSSION
Although the American Association for the Surgery of Trauma’s injury scale was not designed as the treatment guideline, patients with low-grade renal injuries (grades I –III) are dominantly managed nonoperatively, whereas those with high-grade injuries (grades IV–V) have an increased likelihood of surgical intervention [1]. Patients managed nonoperatively had a lower mortality rate, less likely required blood transfusion, and had shorter hospital stay compared with nephrectomy but similar to renorrhaphy [2]. Renorrhaphy can be successfully performed to prevent unnecessary nephrectomy in grade IV renal injuries with hemodynamic instability.
Here, we described a successful renorrhaphy for grade IV renal laceration with unstable hemodynamics after blunt trauma. After controlling the renal pedicle using a vascular clamp (clamping time, 21 min) following the opening of Gerota’s fascia, the renal collecting system was closed using an absorbable suture to provide a watertight seal, and multifocal lacerations in the renal parenchyma were also sutured using pledgeted horizontal mattress sutures. An early decision regarding renal salvageability should be made, and the magnitude of the required reconstructive effort to repair the injury should be determined once hemorrhage is controlled.