Penetrating abdominal injury with a large foreign body following a traffic accident: a case report
Article information
Abstract
Penetrating injuries and blunt injuries present different damage mechanisms. Generally, a blunt injury causes severer damage to tissues and organs than a penetrating injury. We report a case of a penetrating injury involving organ damage due to a large impaled foreign body wherein the penetrating injury was severer than a blunt injury.
Introduction
Penetrating injuries are relatively rarer than blunt injuries among Korean traumatic casualties [1]. Penetrating injuries and blunt injuries typically present different damage mechanisms. Generally, a blunt injury results in severer damage to tissues and organs than a penetrating injury [2]. However, in the present case, the patient sustained a penetrating injury involving organ damage due to a large impaled guardrail section and the injury was severer than a blunt injury.
Case presentation
A 31-year-old man was sent to our regional trauma center after crashing into a guardrail while driving. The patient was conscious, but his initial vital signs were unstable: systolic blood pressure (BP), 67 mmHg; diastolic BP, 38 mmHg; and pulse rate, 98 beats/min. The penetrating injury was observed from the epigastric area to the right flank area of the abdomen (Fig. 1). The patient was immediately shifted to the operating room without imaging, and emergency exploratory laparotomy was performed on suspicion of hemoperitoneum and peritonitis. The intraoperative diagnosis was pancreatic laceration, gastric rupture, and mesenteric rupture due to an impaled guardrail section (Fig. 2). The surgery proceeded as follows: subtotal gastrectomy, Roux-en-Y gastrojejunostomy, primary repair of the pancreas, and bleeder ligation (Fig. 3). Fig. 4 shows the guardrail section that was surgically removed from the patient’s body. Postoperatively, the patient was admitted to the intensive care unit. Subsequently, the patient’s vital signs stabilized and he was transferred to the general ward for conservative management. On postoperative day 80, the patient was discharged in good general condition without any specific symptoms.

The penetrating injury observed from the epigastric area to the right flank area.

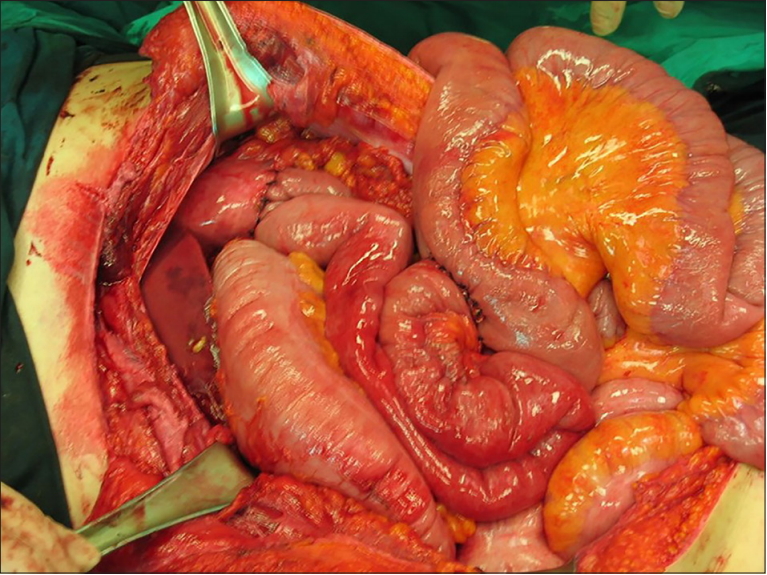
Operative findings: hemoperitoneum and acute peritonitis.
Definitive operative procedure.

The guardrail section surgically removed from the patient’s body
Discussion
Penetrating injuries are the main cause of preventable deaths and are associated with significant morbidity and mortality [3]. Abdominal organs are particularly vulnerable to penetrating injuries, typically characterized by multiple injuries to the gastrointestinal tract, solid organs, and vascular structures [4]. The prognosis of patients with penetrating injuries is variable and depends on the severity of the injury, type of penetration, and time from the trauma to initial treatment [5]. Our report presents a case of penetrating injury caused by a large impaled foreign body. Although the intra-abdominal injury and hemorrhage due to the penetrating injury were severe, the patient survived due to prompt assessment and appropriate emergency surgery.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.