


Introduction
Appendicitis caused by trauma is rare and difficult to predict in the case of patients visiting for severe trauma. In this report, we present a case of a patient who developed acute appendicitis following blunt trauma to the abdomen sustained during a motor vehicle accident.
Case presentation
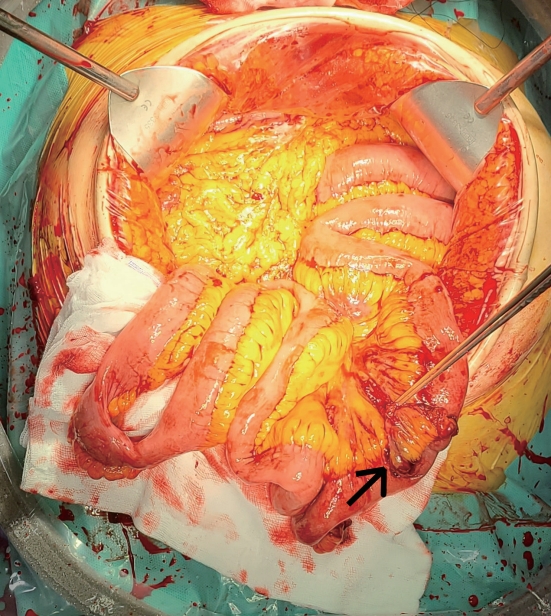
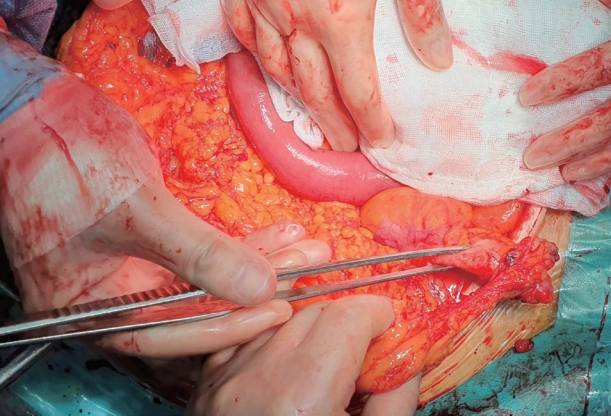
A 68-year-old woman was transferred to our regional trauma center after a motor vehicle accident. The patient was sitting with a fastened seat belt in the passenger seat of a vehicle that was struck on the front end by another vehicle. The patient was conscious, but her vital signs were as follows: blood pressure, 53/26 mmHg; heart rate, 106 bpm; and temperature, 36.5°C. Laboratory investigations revealed hemoglobin (Hb) of 9.8 g/dl and white blood cell count of 13, 370/mm3. Physical examination revealed a distended and diffusely tender abdomen. Extended focused assessment with sonography for trauma (eFAST) showed the presence of peritoneal fluid in the Morison’s pouch. After fluid resuscitation, her blood pressure had risen to 131/53 mmHg, and abdominal computed tomography (CT) scan was performed. The CT scan showed hemoperitoneum around the liver, small bowel mesentery, pelvic cavity, and a dilated appendix with wall enhancement and periappendiceal fat infiltration (Fig. 1). Furthermore, multiple mesenteric tears, small bowel perforation, and a Grade II spleen injury were detected at laparotomy (Fig. 2). On further exploration, acute appendicitis was encountered (Fig. 3). Segmental small bowel resection, splenectomy, and appendectomy were performed (Fig. 4). Postoperatively, the diagnosis of appendicitis was confirmed pathologically. After 13 days, a follow-up CT scan showed a small fluid collection in the intraperitoneal and retroperitoneal spaces and right lower abdominal wall, but no active lesion was evident. The postoperative course was uneventful, and she was discharged on postoperative day 16.
Discussion
Appendicitis typically results from luminal obstruction by miscellaneous factors, including inspissated stool, foreign bodies, and intestinal parasites [1]. Whether appendicitis can be induced by blunt abdominal trauma (BAT) is uncertain, but several theories exist. First, the increased intra-abdominal pressure by BAT increases the lumen pressure of the appendix [2]. Second, blunt trauma might have a direct effect on the appendix with subsequent appendiceal edema and hyperplasia of the intrinsic lymphoid tissues, all of which could result in appendiceal lumen obstruction [3]. Third, hematoma caused by intraperitoneal hemorrhage can produce a significant decrease in visceral arterial blood flow, followed by edema of the bowel wall [4]. Furthermore, many other hypotheses have been raised but because of the lack of cases and absence of verification methods, it is difficult to identify the pathogenesis of trauma-induced appendicitis. Some papers suggest the possibility of preexisting appendicitis just before BAT [5]. In this case, appendicitis occurred before the trauma and was discovered by accident in tests conducted for trauma without the patient knowing it. However, before the trauma, the patient was not diagnosed with any unusual abdominal symptoms, and it is difficult to validate the truth because the operation findings are close to chronic inflammation. If an appendectomy is missed during open surgery, an additional appendectomy can be difficult because of problems such as intestinal edema and adhesion due to the previous surgery.