


Introduction
Postoperative bowel obstruction occurs frequently and may require emergency surgery [1]. About 80% of bowel obstructions are small bowel obstructions, and the main factors are adhesion, incarcerated hernia, and neoplasm [2,3]. The main factors of large bowel obstruction are cancer and adhesion [3-5]. However, it is uncommon not uncommon for two or more factors to occur simultaneously. We report the case of a patient who was diagnosed with colon cancer after undergoing adhesiolysis for adhesive intestinal obstruction.
Case presentation
A 59-year-old man was transferred to our trauma center for postoperative intestinal obstruction that had not improved with nonsurgical treatment for more than 3 weeks. Four years ago, the patient had undergone emergency surgery due to hemopneumoperitoneum from a pedestrian traffic accident. Ileum perforation, cecum serosa tearing, small bowel, and cecal mesentery hematoma were identified intraoperatively, but no active bleeding was found. The patient had undergone ileum primary repair, cecal serosa primary repair, and incidental appendectomy based on the surgeon’s judgment. Postoperative small bowel obstruction occurred after surgery and improved after about 50 days with nonoperative management.
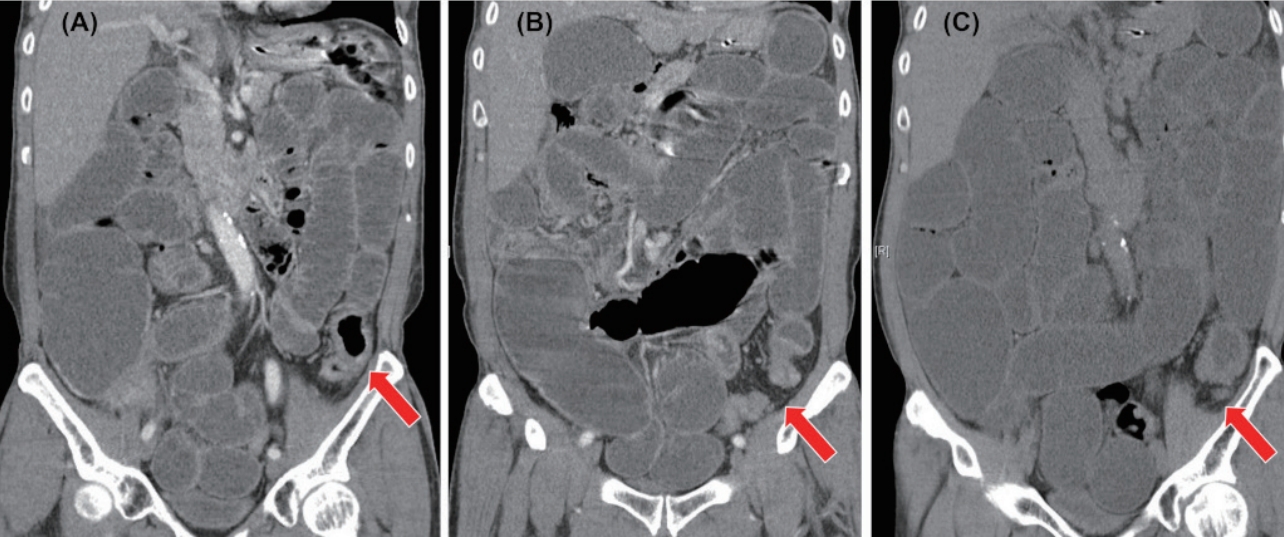
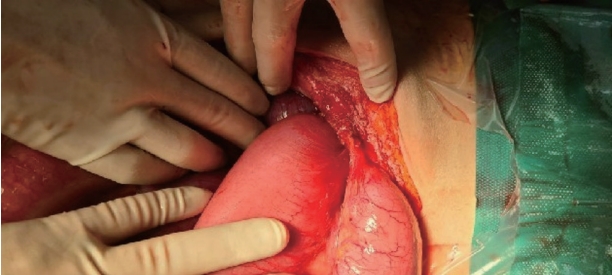
Since then, there had been no history of bowel obstruction. At the time of transfer, there were no laboratory findings that suggested inflammation. Abdominal computed tomography (ACT) showed no findings suggestive of ischemia or necrosis, even though the small and large intestines were dilated; however, an abrupt narrowing site was identified at the descending-sigmoid colon junction (Fig. 1). Regarding ACT, the radiologist did not mention any remarkable findings other than those described above. Surgery was performed for a bowel obstruction that had not improved with a fasting period of 3 weeks or more. At the time of surgery, the small bowel that was positioned 2 cm below the Treitz ligament, which was considered to be the obstruction end-point, was attached to the abdominal wall in a V-shape in the left lower quadrant (Fig. 2). The overall adhesion between the small intestine and the mesentery was checked, and the evaluation of the descending colon was limited to the adhesion. No enlarged lymph nodes were found in the abdominal cavity.
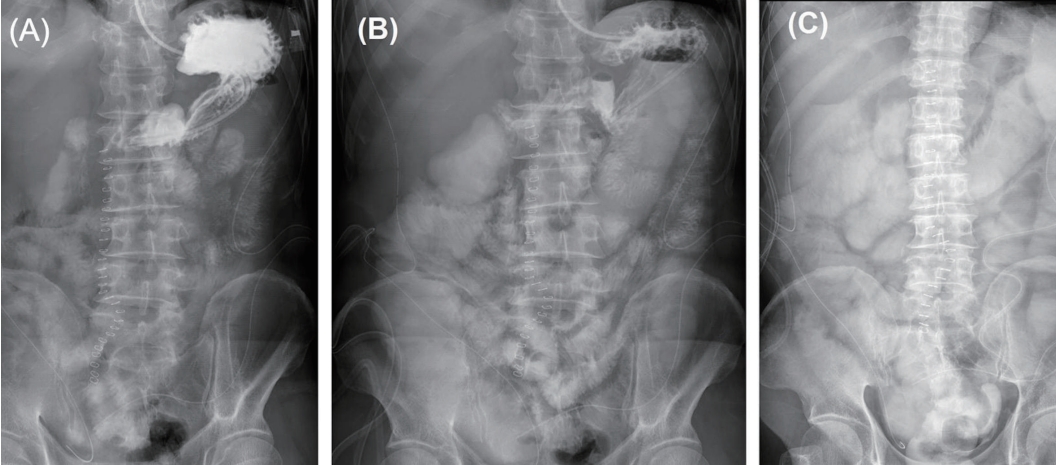
Two weeks after the operation, the patient’s symptoms did not improve; hence, tests for intestinal obstruction were performed. It was confirmed by the small bowel series that part of the intestinal contents was passed (Fig. 3). The narrowing site identified in the previous ACT was seen as the apple core sign in this ACT (Fig. 4). In the sigmoidoscope, a cancer-like lesion obstructed the lumen entirely (Fig. 5); hence, loop transverse colostomy was performed. The patient’s symptoms improved, and the biopsy result of the sigmoidoscope was an adenocarcinoma with moderate differentiation. The patient was managed with neoadjuvant chemotherapy and underwent left hemicolectomy five months later.
Discussion
Adhesion, increased hernia, and large bowel cancer are the main causes of total bowel obstructions [3, 5]. Among them, adhesion is the most common factor and can interfere with the evaluation of other factors during surgery [1-4]. About 60% of large bowel obstructions are cancers [4, 5]. If there is a bowel obstruction, including the large bowel, in a patient without a previous abdominal operation history, the cause is likely to be a cancer. Whenever there is a large bowel obstruction, detailed history taking and evaluation to rule out cancer should be performed, even though the patient has experienced trauma-laparotomy.